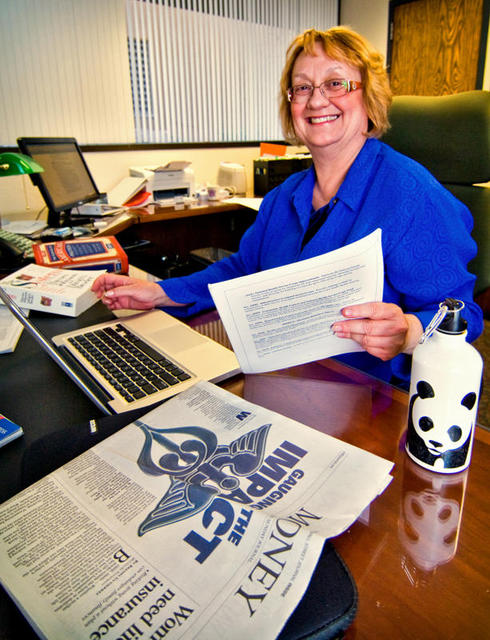
Navigating health reform legislation is no small task. This enormous Patient Protection and Affordable Care Act does everything from impose a 10 percent tax on tanning salon services to reworking the country’s massive Medicare program. That’s why the Alibi turned to health policy expert and seasoned clinician Nancy Ridenour, Ph.D., RN. (Read web extras here, and see a list of basic terms defined here.)She’s the dean of the University of New Mexico’s College of Nursing, and she’s also worked on Capitol Hill as a congressional staffer for the House Ways and Means Committee. There Ridenour helped author portions of the health reform measure. Overall, she says the bill is positive news for the state: “New Mexico is in a good position to benefit."The state’s rural and underserved populations face unique health care challenges. For instance, there will soon be a shortage of primary care providers—a shortage Ridenour describes as “dramatic.” Another big problem is the looming collapse of the Medicare program, which was projected to face bankruptcy by 2017 without reform. The new legislation floats Medicare until 2026. Medicare won’t survive on funding alone. Ridenour points out that the rapidly increasing Medicare population needs a robust number of health care providers. Though the timeline for actually enacting health reform stretches over the next decade, there are immediate provisions to meet the primary care shortage.Ridenour contributed to a provision of the national health reform bill that allows five colleges of nursing to establish residency programs for advanced practice nurses. These nurses have master’s degrees or doctorates, and they often fill similar roles as doctors. The demonstration program will look at how advanced practice nurses can help address the primary care shortage. She says this provision is a huge accomplishment for nursing. “In 2008, there was $9 billion in graduate medical education,” she says. “Very little of that went to nursing.” The health reform measure also cuts funding to the Medicare Advantage plans, which are managed by private insurance companies. The private insurance companies were paid 13 percent more than government-run Medicare. The bill axes that extra 13 percent. "That doesn’t mean people will lose Medicare Advantage," Ridenour says, though some might lose a few perks regular Medicare patients don’t see. Still, Advantage patients might not notice a difference, as some programs weren’t offering any additional services in spite of the extra funding. "We evaluated nationally, and a lot of it was 13 percent extra to the insurance company, not to the participants,” Ridenour says.New Mexico hospitals and providers will also feel some reform-related growing pains. The Kaiser Commission on Medicaid and the Uninsured estimates that 26 percent of non-elderly New Mexicans were uninsured in 2007-2008. Care provided to the uninsured is often uncompensated, and certain hospitals around the state, such as UNMH, care for a larger percentage of the uninsured. These hospitals, known as Disproportionate Share Hospitals, rely on DSH payments from the government to help offset the costs. The health reform legislation will begin to taper these DSH payments.“The idea is that everyone’s going to be covered, so hospitals shouldn’t be needing as much DSH funding," Ridenour says. But there’s a period of time where the DSH cash flow decreases before new money from mandatory insurance rolls in. DSH hospitals are concerned they will lose their government help while they’re still seeing uninsured patients.Once most people are covered after 2014, Ridenour expects New Mexican providers to experience a surge of new patients. Newly covered people will probably need more care up front than average, because they have not had routine maintenance like mammograms or blood pressure checks. This might translate to an initial strain on the system as providers scramble to get everyone caught up with routine care. “And that’s another reason why we need the workforce money, the community health center moneys … to try to bolster up our current primary care and expand it so that we’ll be able to deal with that up front,” she says.Despite challenges, the bill strengthens insurance regulations, extends coverage to 94 percent of the population and makes wellness and preventive care more available and affordable. In November 2009, the Congressional Budget Office estimated that most insured Americans will see their premium rates stay the same or drop. Here in New Mexico’s first congressional district, 18 community health centers will receive $23.4 million to help meet growing primary care demands. Ridenour says the reform bill may seem large and sweeping, but in reality the changes are incremental and build on the existing system. “Any time we’ve tried health reform in the United States, it’s followed similar patterns,” she says. She points to the broad spectrum of political ideologies of U.S. citizens—from universal coverage supporters to advocates of a totally privatized system—as one reason behind the incremental model. That tension of varied beliefs is, she says, "a fiber of our country." But other industrialized nations have been able to go much further with universal coverage. Ridenour adds that the complicated negotiations inherent in the American legislative process are behind the bill’s final form. “Based on what has happened in the last few months, I’m thrilled that something passed because I was starting to think that this wasn’t going to happen at all," she says. "This bill’s just the beginning."
Immediate Provisions
The new health reform legislation means we’ll all be experiencing some changes right away. You’ve probably heard that the first Death Panels are already up and operational here in New Mexico, and yours truly serves as executive executor for ABQ’s very own Bleeding Granny’s Roving Medical Murder Squadron. Here are some other changes you may encounter in the near future:• Pre-existing conditions? Get your swim on! A national high-risk pool designed to provide coverage for people with pre-existing conditions will be theoretically operational 90 days after the bill was passed. • Today’s independence-challenged youth can now stay on Ma and Pa’s insurance plan until age 26. • Insurance companies have to spend between up to 85 percent of their blood money—I mean premium payments—on providing services to beneficiaries. Money not spent on services must be rebated. • Seniors will find a $250 hidden in the “donut hole” of their Medicare Part D prescription drug coverage gap. • Medicaid recipients will see increased drug rebates. • The bill establishes the Patient-Centered Outcomes Research Institute to support comparative effectiveness research, which indirectly improves national sleep habits through boredom-induced napping.• A Workforce Advisory Committee will address primary care and nursing shortages. • Medicare payments will support primary care residency programs in federally qualified health centers.